Michael J. Paidas, MD
- Associate Professor
- Co-Director, Yale Women and Children? Center for Blood Disorders
- Co-Director, National Hemophilia Foundation?Baxter
- Clinical Fellowship Program at Yale
- Division of Maternal- Fetal Medicine
- Department of Obstetrics, Gynecology, and
- Reproductive Sciences
- Yale University School of Medicine
- New Haven, Connecticut
Montelukast dosages: 10 mg, 5 mg, 4 mg
Montelukast packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

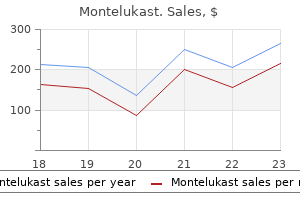
Montelukast 5mg lowest price
The high quality of the skin usually varies from normal with pimples and hyperhidrosis being distinguished options. Fusion and malformation of other joints, together with the elbows and shoulders, usually occur. The quality of the skin typically varies from normal, with zits and hyperhidrosis being prominent features. It must be noted that different researchers have studied the intracranial quantity of youngsters born with craniosynostosis. We found them to have cranial vault lengths averaging solely 87% of the age-matched norms. The medial orbital partitions were (horizontally) short at 87% of normal, whereas the extent of globe protrusion was extreme at 134% of agematched norms. These findings confirmed horizontal (anteroposterior) deficiency of the upper and midface. The imply cranial size initially achieved (after monobloc osteotomy) was 98%, and at 1 year, it was 92% of the management worth. When compared with age-matched controls, the orbital measurements mirrored improvement in the midorbital hypertelorism (midinterorbital width was 97% initially after operation and 102% at 1 yr) and orbital proptosis (early after surgical procedure, 86% of values for age-matched normal youngsters; 92% at 1 yr). The medial orbital wall length initially normalized at 101% and later at 97% of regular values. The zygomatic arch size initially corrected at 106% and later to 101% of normal. The major targets at this stage are to decompress the brain and provide elevated space for it within the anterior cranial vault and to enhance the orbital volume to decrease globe protrusion. She was raised in Athens, Greece, and was unable to endure craniofacial or extremity reconstruction. When utilizing the facial bipartition strategy, a extra normal arc of rotation of the midface complex is achieved with the midline cut up. This further reduces the stigmata of the preoperative "flat, wide, and retrusive" facial appearance. The facial bipartition also permits the orbits and zygomatic buttresses as items to shift to the midline (correction of hypertelorism) while the maxillary arch is concurrently widened. Horizontal development of the reassembled midface complex is then achieved to normalize the orbital depth and zygomatic length. The forehead is generally flat, tall, and retruded, with a constricting band simply above the supraorbital ridge, giving the impression of bitemporal narrowing. Note that stabilization was achieved with cranial bone grafts and plate and screw fixation. O and P, Frontal and profile views three years after first stage cranio-orbital reshaping; additional staged reconstruction is required. The anterior cranial vault width (intercoronal distance) has remained secure at one hundred fifteen mm. The anterior interorbital distance diminished from 29 to 25 mm, which nonetheless represented 137% of the age-matched management worth. A Le Fort I osteotomy is required to permit for horizontal development, transverse widening, and vertical adjustment together with an osteoplastic genioplasty to vertically scale back and horizontally advance the chin, often mixed with bilateral sagittal break up osteotomies of the mandible. The elective orthognathic surgical procedure is carried out in conjunction with detailed orthodontic treatment deliberate for completion on the time of early skeletal maturity (~13�15 yr in ladies and 15�17 yr in boys). At 18 months of age, she returned with turricephaly and a constricted anterior cranial vault requiring further cranio-orbital decompression and reshaping. At 5 years of age, she underwent anterior cranial vault and facial bipartition osteotomies with reshaping. As a part of her staged reconstruction, she would require orthognathic surgical procedure and orthodontic therapy deliberate for the teenage years. A, Frontal view at eight months of age after a lateral canthal development procedure with residual deformity. G, Frontal view at 5 years of age simply earlier than further anterior cranial vault and facial bipartition osteotomies.
Purchase montelukast no prescription
The function of the superior head of the lateral pterygoid muscle is predominantly involved with closing actions of the jaw and with retrusion and ipsilateral movement. A abstract of the actions of the lateral pterygoid muscle and the other supramandibular muscles is given in Table 47-1. Inframandibular Muscle Group the inframandibular muscles can be subdivided in to two teams: the suprahyoids and the infrahyoids. The suprahyoid group consists of the digastric, geniohyoid, mylohyoid, and stylohyoid muscle tissue; lies between the mandible and the hyoid bone; and serves to both increase the hyoid bone, if the mandible is fastened in position by the supramandibular group, or depress the mandible, if the hyoid bone is mounted in position by the infrahyoids. The infrahyoid group, consisting of the sternohyoid, omohyoid, sternothyroid, and thyrohyoid muscle tissue, attaches to the hyoid bone superiorly and to the sternum, clavicle, and scapula inferiorly. This group of muscles can both depress the hyoid bone or hold the hyoid bone in place, relative to the trunk, throughout opening movements of the mandible. Articular issues, typically accompanied by inside derangement, include noninflammatory and inflammatory arthropathies, development problems, and connective tissue problems. The inferior joints, consisting of the condyle and disk, are responsible for rotation, a hingelike motion. The middle of rotation is taken into account to be along a horizontal axis passing through each condyles. Nevertheless, most mandibular actions are translatory as well, involving a gliding motion between the disk and the temporal fossa, which are the parts of the superior joints. The necessary function of the supramandibular and inframandibular muscle groups on mandibular motion and function is clear in these situations. Such therapies embody occlusal adjustments (for gross discrepancies), night-guard home equipment (for joint unloading, jaw repositioning, and occlusal protection), nonsteroidal anti-inflammatory drugs, muscle relaxants, and bodily therapy. Fibromyalgia is a systemic condition marked by poor sleep, generalized ache with absence of localization to joints, and a historical past of somatization in different organ methods corresponding to irritable bowel syndrome and headaches. Myotonic dystrophy is a dominantly inherited multisystem dysfunction that may affect facial muscular tissues in absolutely developed illness states. They are inclined to exert their pathologic effects in comparable style, typically leading to trismus, lack of perform, and pain. Myositis ossificans progressiva is a uncommon situation leading to fibrosis of sentimental tissues after obvious minor trauma. Osteoarthrosis can manifest as chondromalacia (softening of the cartilage), momentary or permanent disk displacement, degenerative changes within bone and cartilage usually with osteophyte formation and reworking, fibrosis, or any combination of those. Noninflammatory arthropathies are distinctly limited in their quantity of overt irritation and may be clinically silent or focal in nature. These proteases (aspartic, cysteine, serine, and metalloproteases, amongst others) function at low and impartial pH to exert their pathologic effects resulting in degenerative modifications. The presence of free radicals has been postulated as an amplifying issue within the activation of cytokines, enzymes, neuropeptides, and arachidonic acid metabolites resulting in degenerative joint disease. Nitric oxide has direct results on prostaglandin synthesis and cyclooxygenase-2 enzymes resulting in synovial inflammation and tissue destruction. In symptomatic joints, catabolic processes have been found to exert higher total results, thus disrupting the balance between anabolic physiologic maintenance and the unfavorable results of catabolic cytokines. Multiple unbiased research support the speculation of catabolic imbalance within the joint. These findings correlated with elevated ranges of keratan sulfate in the synovial fluid of those joints, suggesting its position as a potential biochemical marker for articular cartilage degradation. Inflammatory arthropathies are primarily because of such conditions as rheumatoid arthritis, juvenile rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, or arthritis resulting from infectious causes (see Table 47-2). Secondary causes of inflammatory arthropathies embody synovitis, capsulitis, traumatic arthritis, or acute inflamed crystal-induced arthritis, corresponding to gout. As mentioned previously, noninflammatory arthropathies can progress to the inflammatory sorts via increasing concentrations of degradation products within the joint. Historically, the gross evaluation of disk position and disk integrity has been the mainstay of inside derangement analysis and administration. More lately, the physiologic exercise of synovial cells, chondrocytes, and inflammatory cells in symptomatic joints has been related to pathogenesis. Osteoclast differentiation requires cell-to-cell contact between osteoclast progenitors and bone marrow stromal cells.
Diseases
- Perilymphatic fistula
- Hyperornithinemia, hyperammonemia, homocitrullinuria syndrome
- Subcortical laminar heterotopia
- Cystic fibrosis gastritis megaloblastic anemia
- Salivary disorder
- Holoprosencephaly deletion 2p
Cheap 5 mg montelukast overnight delivery
Proper alignment and occlusion are then attained, and the segments are stabilized with appropriate transosseous wire or a small (2. A, Subluxed tooth and alveolar fracture associated with maxillary left central incisors. Traumatized tooth are placed in to preinjury alignment, acid-etched, and stabilized with composite resin. A, Blunt facial trauma leading to alveolar fracture and perioral delicate tissue lacerations. B, Occlusal radiograph confirms alveolar fracture with lingual displacement ("apical lock") of mandibular central incisors and left lateral incisors (arrow). Stabilize enamel which may be cell in the fractured segment with an applicable secondary splint after bony stabilization. Likewise, keep away from eradicating teeth that are considered nonsalvageable and which are throughout the bony phase till the bony therapeutic phase is completed (~4 wk). Successful remedy of alveolar fractures is associated with the pulpal healing after the harm. When the fracture stage is apical to the root suggestions, the vascular provide to the pulp is much less at risk; nevertheless, if the road of the fracture and root apices are in contact, the tooth in the alveolar section are at a better danger for internal or exterior resorption. In concomitant accidents, corresponding to maxillary or mandibular fractures, early maxillomandibular fixation is completed with a method that will permit for dual treatment of the dental and/or alveolar harm and the jaw damage. Aim treatment at soft tissue protection in the form of even handed mucosal advancement flaps. Inspect the wound for possible overseas physique (asphalt) accumulation, which might lead to unsightly unintentional tattooing. If present, perform meticulous removing inside 12 hours, with care to not further inoculate the affected person. Contusion A contusion, a hemorrhage of subcutaneous tissue without laceration or break of overlying gentle tissue, is much like a bruising damage caused by blunt trauma. This damage could additionally be related to an underlying hematoma or ecchymotic formation, which is mostly self-limiting. Remove devitalized tissue in a conservative method, and suture in a way that limits wound tension. More critical avulsive gingival wounds warrant close inspection of remaining tissue and underlying bony integrity. Exposure of any underlying bony defect may point out localized keratinized sliding or development flaps. Treatment of Trauma to the Gingiva and Alveolar Mucosa Traumatic damage to the oral gentle tissue mainly consists of abrasion, contusion, and laceration. Abrasion An abrasion is a superficial wound whereby the epithelial or gingival tissue is rubbed, worn, or scratched. Treatment consists of local cleaning with a light disinfectant cleaning soap for the pores and skin and saline rinsing and/or irrigation of the gingiva. Managing the affected person may require sedation and restraint; thus, further components must be handled through the remedy routine. Displacement accidents are extra prevalent than are tooth fractures in the major dentition secondary to the relative resilience of the encompassing bone. Note the "buccal-occlusal" and "buccal-incisal" place of the primary roots (arrow). Luxations Subluxation Lateral luxations Extrusion Intrusion are extra frequent within the pediatric dentition than within the permanent dentition. Andreasen and Ravn59 reported on the overall prognosis of the traumatized everlasting successors, secondary to forces applied by the first dentition. Association of the type of luxation harm with respect to the malformation of the everlasting dentition. The Relationship of Internal Protection Devices to Athletic Injuries and Athletic Performance. Influence of maturation standing and tooth kind of everlasting tooth upon electrometric and thermal pulp testing. Epidemiology of traumatic dental injuries to main and permanent enamel in a Danish inhabitants pattern. Luxation of permanent tooth because of trauma: a clinical and radiographic follow-up study of 189 injured teeth.
Discount montelukast 10mg on line
Full-mouth rehabilitation could also be needed to reestablish proper anterior steering and dental relationships. Greater numbers of implants could additionally be planned as properly as avoiding narrower-diameter implants, especially in posterior areas. For instance, if both arches are restored, porcelain in opposition to porcelain occlusion is discouraged. The affected person was rehabilitated with maxillary and mandibular mounted hybrid (acrylic to metal) prostheses. It is well-known that conventional denture wearers have decrease most chew forces than dentate topics. Therefore, therapy plans for tooth alternative towards an opposing complete denture could additionally be much less mechanically demanding than pure dentition. Implant prostheses have been proven to improve masticatory perform and biting drive. However, generalizations could also be made primarily based on biomechanical assist, long-term studies, and medical expertise. When the minimum variety of implants is used, the prosthesis is positioned at risk if a complication happens. The philosophy of "defend the prosthesis" is a prudent guideline in treatment planning and designing of the implant support system. With increased atrophy, less bone is available for implant placement and fewer residual ridge for prosthetic assist. As such, using solely two implants could not present the desired improvement in denture function. In addition, higher masses are positioned on the 2 independent implants in softer high quality bone. Although the fee is decrease, in contrast with that of utilizing a connecting bar, the mechanical advantage of implant splinting is most popular. The prescription of an overdenture is usually an unplanned various when issues forestall the consideration of a exhausting and fast prosthesis. The minimal variety of implants for help of a maxillary the chance of fracture and impact forces. The benefit of a detachable implant prosthesis is that it might be taken out at evening to avoid nocturnal forces. The muscular tissues of mastication generate the occlusal forces positioned on the implant system. Several components affect masticatory dynamics together with affected person size, gender, age, and skeletal relationships. Older sufferers sometimes report decrease biting forces than youthful sufferers, and the chew drive of men is on average 30% greater than ladies. A chew splint is used to defend the implant connecting bar and opposing dentition from nocturnal parafunctional exercise. A maxillary overdenture with six implants could additionally be removable yet completely implantsupported. The four maxillary implants planned for overdenture help are placed anterior to the sinuses. The maxillary overdenture is retained by the attachments and supported by the bar in addition to the palate and posterior ridges. A maxillary overdenture supported by six implants is completely implant-supported with no palatal coverage and retained with attachments. The minimum number of implants proposed for help of a maxillary mounted prosthesis is 4. Although the early Swedish literature documented maxillary instances with as few as four implants, they more usually recommended six. Although this approach has shown favorable early results, the apparent important disadvantage is that the lack of one implant results in complete prosthetic failure. Greater numbers of implants (7�12) may be recommended when mechanical risk elements are higher, bone quantity is compromised, and/or bone density is poor. Two separate implant bars are discouraged because the maxillary overdenture has a tendency to tilt with anterior biting forces.
Discount montelukast 4 mg line
Damage to the crest right now might lead to disturbance in progress and cosmetic deformity of the crest; nevertheless, splitting the crest longitudinally, which permits entry to the underlying cancellous marrow, has been used for harvest of bone in this age group with no reported development alteration and fewer postoperative gait disturbance than with the lateral subcrestal strategy. Bone grafts consisting of diploic bone have been shown to be extra profitable than these grafts harvested using a high-speed rotary gadget to shave off primarily cortical bone from the floor of the calvarium. In one research in which primarily diploic bone was rigorously harvested from the calvarium, the results were still less profitable (80% graft success) than with traditional iliac crest bone (93% graft success). This limitation may render calvaria as a much less helpful source for big clefts and bilateral clefts. In main bone grafting, the rib is the only web site for sufficient quantity of bone with acceptable morbidity. These choices would also be possible sources for bone for late secondary grafting, in addition to grafts from the mandibular symphysis and probably the tibia. Because the info counsel that grafting through the combined dentition is good, discussion focuses on comparing varied sources of graft materials for this group of sufferers. The benefits and downsides of various potential sources of bone are outlined in Table 44-3. Iliac Crest Potential benefits of the iliac crest bone graft embody low morbidity and excessive volume of viable osteoblastic cells (cancellous bone); two groups may fit concurrently, and this process is properly accepted by the affected person. The buccal development flaps, palatal flaps, and nasal ground are developed followed by restore of the nasal flooring and palatal tissue. The patient will doubtless have a shorter hospital keep as a outcome of less postoperative ache. Complications at a secondary surgical site are eliminated and total surgical time may be shortened. In addition, the dearth of structural integrity of the absorbable collagen sponge can lead to an unsupported ala. At this point in time, plainly even with the benefits that include avoiding a secondary surgical site, autogenous bone grafts for the reconstruction of alveolar clefts continues to be the gold standard. Grafting from the iliac crest if two teams are used can decrease total working time compared with calvarial grafting. Lastly, the incision for graft harvest is hidden within the hairline, which can have a cosmetic advantage. There is a perceived elevated danger by patients and their families, although several research show that the morbidity of bone harvest from the calvaria is minimal. Allogeneic Bone In an effort to remove the morbidity and time necessary to harvest bone from any autogenous site, some authors have evaluated allogeneic bone as a possible supply of graft material. Studies have proven that allogeneic bone can be used successfully to graft secondary alveolar cleft defects and that outcomes can be in contrast favorably with these achieved with autogenous bone. In basic, bone therapeutic with autogenous bone is biologically different than with allogeneic bone. Autogenous bone grafts provoke an angioblastic response early within the therapeutic process, and some of the transplanted cells remain viable, resulting in a more speedy formation of recent bone. In distinction, allogeneic bone grafts demonstrate slower revascularization, because no viable cells are transferred with the graft. Mathematically, the chance is quite small but could also be of concern to sufferers and households. The potential benefits of avoiding a secondary surgical web site and obtaining the same outcomes as these with autogenous grafting have prompted surgeons to use the fabric in quite so much of maxillofacial bony defects. The mature bone quantity obtained in both teams was measured by comparing Pre-versus Postsurgical Orthodontics Controversy exists concerning the utilization of orthopedic expansion of the cleft segments and the connection between enlargement and grafting. Most authors favor presurgical growth, citing simpler expansion because of less resistance, improved access to the cleft for closure of the nasal flooring, higher postoperative hygiene, and fewer chance of reopening the oronasal fistula. Expansion of the lesser section will bring the arch in to better kind and facilitate grafting with out widening the cleft. Proponents of growth after grafting cite advantages of improved bone consolidation when the graft is placed under a dynamic load throughout therapeutic, a smaller soft tissue defect to close, much less issue in procuring an adequate quantity of bone, and a narrower defect, which will regenerate bone extra shortly. In these instances, the tip level of presurgical enlargement is improved arch kind, not necessarily decision of crossbite. Bilateral clefts with collapse of the lateral segments may benefit from presurgical expansion. A, Occlusal photograph of bilateral cleft with collapse of the lateral segments and protrusion of the premaxilla. D, Expansion of the bilateral cleft permits the premaxilla to move posteriorly and improves arch type and alignment of the segments.
Order montelukast with a mastercard
A, Outline of a nasolabial flap in a affected person with a defect within the anterior floor of the mouth. The flap is equipped by the angular artery, intraorbital artery, and infratrochlear artery and can be based mostly either superiorly or inferiorly. The space of recruitment for nasal reconstruction is in nearer proximity to the primary defect than is the forehead flap. When the pedicle is divided, the defect could be closed primarily by inserting the scar within the nasal facial junction and the nasolabial flap fold. The labial artery supplies the flap and ought to be maintained with a small cuff of subcutaneous tissue and muscle surrounding the vascular pedicle. They use adjoining tissue, have a wonderful blood supply, and are related to minimal morbidity. The tongue has wonderful axial and collateral circulation, with the lingual artery providing the primary blood supply. Up to one half of the tongue could be rotated for tissue coverage without compromising speech, mastication, or deglutition. A B Regional Flaps For giant facial defects, native flaps might not present enough tissue to adequately restore the missing tissue. They are regularly harvested from the neck, chest, or axilla and can present protection of enormous surface areas on the face. Selection of a specific regional flap depends on the dimensions and placement of the defect and in addition on the intrinsic properties of the flap. Advantages of regional flaps embrace the large quantity of sentimental tissue and skin obtainable. Disadvantages of these type of flaps embrace poor colour and texture match, extreme bulkiness of the flap, and donor web site morbidity. Pectoralis Major Myocutaneous Flap the pectoralis major myocutaneous flap remains a workhorse of reconstructive surgery38�40 the flap was launched by Ariyan41 and has supplied a dependable technique of soft tissue reconstruction of bone and delicate tissue defects of the mandible and maxilla. A, Patient with a traumatic lip deformity with avulsion of a portion of his higher lip. B, Reapproximation of the orbicularis oris muscles and perialar advancement flaps to reestablish higher lip size. A and B, Use of an anteriorly based tongue flap to cover the soft tissue deficit resulting from an alveolar cleft. The thoracoacromial artery arises from the second portion of the axillary artery and varieties 4 branches because it penetrates the fascia. The pectoral branch is the most important artery that provides the pectoralis major myocutaneous flap. The position of the vascular pedicle may be approximated by drawing a line from the shoulder point to the xiphoid. The pectoral branch descends at a proper angle from the middle of the clavicle until it meets this line. Branches of the interior mammary artery provide the medial portion of the muscle and skin over the sternum. The flap provides good coverage for the carotid artery when combined with a neck dissection. The pectoralis main myocutaneous flap is split lateral to the inner mammary artery perforating vessels. The muscle may be divided lateral to the skin island to go away the lateral portion of the muscle intact; this preserves the axillary fold. This fascia is equipped by the center temporal vessel, which originates just under the zygomatic arch. The temporalis muscle is provided by both the anterior and the posterior deep temporal arteries, which come up from the second portion of the internal maxillary artery. A, Temporalis muscle flap for restore of a midface defect brought on by a shotgun wound.
Dalmation Insect Flowers (Pyrethrum). Montelukast.
- What is Pyrethrum?
- What other names is Pyrethrum known by?
- Are there safety concerns?
- How does Pyrethrum work?
- Head lice and crablice infestations.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96401
Proven 4mg montelukast
Extracapsular condylar fractures are greatest handled with a nonchew food regimen and closed reduction with elastic steering in younger youngsters, permitting managed function and comfort. Open reduction and inside fixation is reserved for selected younger youngsters and adolescents. It is felt by some that weakening and supreme resorption of the fixation plates within 1 year will end in much less progress disturbances and normalize the mineralization dynamic of the mandible. Right mandibular body fracture in a 14-year-old with momentary intermaxillary fixation and a single resorbable fixation plate. The anterior main dentition has shortened root structure, lending itself to fracture, intrusion, concussion, subluxation, partial avulsion, and full avulsion injuries. Comprehensive evaluation should try and account for lacking and probably swallowed or aspirated enamel, especially in obtunded patients. Plain films are helpful to rule out the presence of foreign bodies inside wounded soft tissues. Luxated or avulsed adult enamel must be repositioned and re-implanted, ideally within 60 minutes. Dentoalveolar segment fractures can usually be lowered and stabilized with arch bars or wires, as in luxated or avulsed teeth accidents. Larger alveolar segments might best be treated by plate and screw fixation, especially if tooth are significantly fractured or absent. Interval analysis by a pediatric dentist is sometimes recommended to evaluate for the need of house maintenance and longitudinal monitoring of dental improvement. B, Placement of a single resorbable fixation plate across the mandibular body fracture. Adolescent fracture management mirrors that of adults, but follow-up for progress perturbations ought to be documented in to the early grownup years especially for mandibular condylar fractures. Generally, three primary areas of growth could also be affected by injuries: the orbital region, the nasomaxillary advanced, and the condylar-ramal components. Fractures of the orbital region in very younger kids could result in periorbital tissue atrophy and subsequent orbital volume loss, notably in a crush harm. It is necessary to rigorously and completely evaluate this with the parents and advise long-term follow-up throughout growth. Condylar fractures contain the mandibular progress heart and will lead to long-term development abnormalities through growth restriction and growth of a malocclusion and lower facial third facial asymmetry or deformity. Also, degenerative modifications are prone to occur, resulting in early-onset arthritis at the temporomandibular joint. Unlike grownup condylar fractures, youngsters have the capability for condylar transforming and complete recovery of type and performance. Policy Statement of the American Academy of Pediatrics, Committee on Pediatric Emergency Medicine. There has been a shift of trauma incidence to the younger population owing to elevated independence of children and risk-taking behavior amongst youth, significantly in adolescence, which puts children in danger for significant damage. Children require fast intervention in trauma care, including facial accidents, to protect tissue health and optimum outcomes. Facial accidents are generally age-dependent in that cranio-orbital accidents are seen extra in the very younger whereas midface and decrease face injuries are seen more frequently within the older and adolescent baby. Particular attention to gentle tissue management of the eye, nasal, and ear areas, including neurovascular entities, requires preservation of tissue, focused restore, assist of repaired buildings, and scar administration modalities to be able to obtain a great lead to kind and function. Fracture management within the very young has undergone latest change with the advent of resorbable fixation supplies and techniques as properly as the increased appreciation for skeletal response to trauma, significantly for long-term facial improvement. Post-traumatic obstruction of lacrimal pathways: a retrospective evaluation of 58 consecutive naso-orbitoethmoid fractures. Toxic-shock syndrome associated with nasal packing: analogy to tampon-associated illness. Absorbable versus nonabsorbable sutures within the management of traumatic lacerations and surgical wounds. The impact of silicone gel on fundamental fibroblast growth issue levels in fibroblast cell tradition.
Purchase 10 mg montelukast with mastercard
Sural grafts up to 20 cm in size are potential, and patients tolerate the donor website deficit well. As a branch of the cervical plexus (C1, C2), the greater auricular nerve supplies sensation to the pre- and postauricular areas, the decrease third of the ear, and the skin overlying the posteroinferior border on the angle of the mandible. Patients are generally not amenable to sacrificing sensation of 1 facial area to regain sensation in another neighboring location. The sole benefit of a higher auricular graft over a sural graft is in conditions when it might be harvested by way of the same incision for another procedure, such because the restore of an extraoral mandibular fracture or administration of pathology. The fundamental premise with graft repair is that the nerve graft will provide the Schwann cell conduit sheaths and the growth elements necessary to help and encourage axonal sprouting by way of the graft towards the target web site. This allograft is avialble in varied lengths and diameters that can be utilized for the trigeminal system. Although the allograft is decellularized, it mainatins certain neurotrophic and neurotropic factors such as basement membrane laminin. It should be remembered that a poor end result after tried microneurosurgery might preclude future surgical choices; therefore, the best likelihood for microneurosurgical success happens at the first (and most likely, last) surgical intervention. In common, the nerve regeneration course of progresses at approximately 1 mm/day (~3 cm/mo) from the cell body to the goal web site. With graft or conduit oblique restore, the time-frame is lengthened owing to slowed regeneration through the graft web site, and recovery is variable. All nerve injuries must be documented and evaluated with a history, examination, and neurosensory testing (objective and subjective). In cases of observed or identified nerve injury, prompt referral for microsurgery offers one of the best alternative for sensory recovery. Complete recovery in 1 month signifies neurapraxia, and no further therapy is indicated. Neurosensory dysfunction that lasts longer than 1 month indicates a higher-grade injury with uncertain spontaneous neurosensory restoration. Nerve injuries that show improvement (objective and/or subjective) could additionally be followed up expectantly. Most nerve accidents resolve inside 3 to 9 months, however provided that enchancment begins earlier than 3 months. Some painful neuropathies may be managed nonsurgically under the supervision of a microneurosurgeon or different skilled individual. Angry uninformed sufferers with nerve accidents are less more likely to enhance with any remedy, surgical or nonsurgical. A dialogue concerning choices and the chance of nerve damage should be provided so that the patient can provide informed consent. Surgery delayed beyond 12 months is critically compromised by distal nerve degeneration and the development of persistent pain syndromes. The etiology of altered sensation in the inferior alveolar, lingual, and psychological nerve on account of dental treatment. Lingual flap retraction and prevention of lingual nerve damage related to third molar surgery: a scientific evaluate of the literature. Dysesthesia of the lingual and inferior alveolar nerves following third molar surgery. Sensory impairment of the lingual and inferior alveolar nerves following removing of impacted third molars. Incidence of nerve harm following third molar removing: a West Scotland Oral Surgery Research Group examine. Inferior alveolar nerve damage after decrease third molar surgical extraction: a prospective study of 1117 surgical extractions. Clinical and anatomic observations on the relationship of the lingual nerve to the mandibular third molar area. The relationship of the lingual nerve to the mandibular third molar region: an anatomic examine. Anatomic position of the lingual nerve in the mandibular third molar region with special consideration of an atrophied mandibular crest: an anatomical examine. Incidence of lingual nerve trauma and postinjection issues in standard mandibular block anesthesia. Lingual nerve dam, age as a result of inferior alveolar nerve blocks: a attainable rationalization. Letter: prolonged paraesthesia following inferior alveolar nerve block using articaine.
5 mg montelukast overnight delivery
H, Same view after osteotomies, reshaping, and stabilization of bone segments with miniplates and screws. These lateral orbital step-offs are unattractive and are seen to the casual observer at conversational distance. Surgical modification performed later is difficult, often with less than best aesthetic results. O, Comparison of lateral cephalometric radiographs before and after reconstruction. Morphologic outcomes achieved in these children 1 yr after present process a basic suture launch and anterior cranial vault and higher orbital procedure, designed to decompress and reshape these regions, have been also evaluated. In comparability with agematched controls, orbital measurements revealed a widened anterior interorbital width at 122% of regular, an elevated intertemporal width at 121% of regular, globe protrusion at 119% of normal, and a short medial orbital wall size at solely 86% of regular. The distance between the zygomatic buttresses and the interarch widths had been found to be increased at 106% and 103% of regular, respectively. The zygomatic arch lengths were substantially shortened at solely 87% of the values of age-matched controls. These findings confirmed clinical observations of brachycephalic anterior cranial vaults with shallow, frequently hyperteloric orbits and globe proptosis. The intracranial volumes additionally had been in contrast with those of an age- and gender-matched cohort, and we also reviewed the rate of cranial enlargement with growth. When comparing postoperative volumes with the normative information, all 13 maintained volumes at or larger than the mean. Psychosocial concerns also assist the upper midface and ultimate cranial vault process taking place in patients 5 to 7 years of age. When the procedure is carried out at this age, the child might enter the primary grade with a chance for satisfactory vanity. Routine orthognathic surgical procedure might be essential at the time of skeletal maturity to obtain a perfect occlusion, facial profile, and smile. A Le Fort I osteotomy to allow for horizontal advancement, transverse widening, and vertical adjustment is usually required together with an osteoplastic genioplasty (vertical reduction and horizontal advancement) to further correct the lower face deformity. Secondary deformities of the mandible ought to be concurrently corrected via sagittal cut up ramus osteotomies. When he was 11 years of age, the affected person was seen by one other surgeon and underwent a Le Fort osteotomy with development by way of an extracranial method. He presented in his late teenage years with asymmetrical and dystopic orbits, zygomatic hypoplasia, a retrusive higher jaw, an asymmetrical lower jaw, and an extended chin. He underwent a mixed orthodontic and orthognathic method, together with a Le Fort I osteotomy (horizontal advancement), bilateral sagittal cut up osteotomies of the mandible (correction of asymmetry), and an osteoplastic genioplasty (vertical discount and horizontal advancement). During the identical common anesthesia procedure, he underwent a reopening of his coronal (scalp) incision with harvesting of break up cranial grafts to recontour and increase the orbits and zygomas. H, Craniofacial morphology with deliberate and accomplished osteotomies and reconstruction. The sequence included seven ladies and one boy, with an average age at surgery of 12 months (range, 9�23 mo). The average postoperative follow-up interval was 34 months (range, 12�48 mo) at the shut of the examine. Significant preoperative morphologic findings included a large anterior cranial vault at 110% of normal, a maximum cranial length that averaged solely 90% of regular, a considerably widened anterior interorbital width at 117% of regular, an increased lateral interorbital distance at 112% of regular, and a widened bitemporal width at 122% of normal. Globe protrusion was significant at 121% of regular, and the medial orbital wall size was less than regular at 92%. In the upper midface (zygomatic) area, each the width between the zygomatic buttresses and the interarch width have been discovered to be elevated at 109% of regular, whereas the zygomatic arch lengths have been considerably shortened at 79% of regular. The measurements confirmed the scientific observations of brachycephalic, hyperteloric anterior cranial vaults, orbits, and zygomas, accompanied by eye proptosis and midface deficiency. There were no infections, wound difficulties, or central nervous system or ophthalmologic sequelae after any of the operations performed. One toddler suffered intraoperative cardiac arrest due to intravascular quantity depletion; the arrest responded to closed-chest cardiac therapeutic massage and blood transfusion.
Discount montelukast 4 mg on-line
If this means that two plates are essential to achieve absolute rigidity, they need to be used. If it implies that a larger compression plate want be utilized, that should also be carried out. There is little question that the addition of a second level of fixation provides more stability to the fracture. However, to take mechanical benefit of a couple of level of fixation, the fixation units should be positioned as far apart as attainable. Because fixation units are applied to the lateral floor of the mandible, the ability to use two-point fixation requires that there be adequate top of bone so that the fixation units can be positioned far aside. If one chooses to use two load-sharing bone plates to provide rigid fixation, one have to be cognizant of the place of the tooth roots and the inferior alveolar/mental nerves. Depending on the size of the plate and whether or not or not an arch bar may also be used to provide one other level of fixation, the fixation might be rigid or functionally steady. These plates perform as inside fixators, reaching stability by locking the screw to the plate. Conventional bone plate�screw systems require exact adaptation of the plate to the underlying bone. Without this intimate contact, tightening of the screws will draw the bone segments towards the plate, leading to alterations within the place of the osseous segments and the occlusal relationship. Locking plate�screw techniques provide certain advantages over different plates in this regard. The most important advantage may be that it turns into pointless for the plate to intimately contact the underlying bone in all areas. A and B demonstrate biomechanical effectiveness of two plates when placed at totally different distances from one another. This assemble is way much less steady than the one in A due to the limited house between the 2 plates, regardless of the fact that the identical two bone plates are utilized. C and D demonstrate biomechanical effectiveness of two constructs when just one plate is applied. D, A single plate is utilized to a assemble with a higher vertical height (Ht a). The assemble with a higher vertical dimension (D) is rather more secure because of the higher buttressing impact provided by the longer moment arm of the elevated vertical dimension of bone. Use of a single robust bone plate (reconstruction plate) when the vertical height of the mandible is small. Compression plates help to decrease the fracture hole and to impart stability by the frictional interlock they induce. This theoretical benefit is certainly more essential when utilizing large bone plates, such as reconstruction plates, which may be very troublesome to perfectly adapt to the contours of the bone. Another theoretical benefit to the use of locking bone plate�screw methods is that the screws are unlikely to loosen from the bone. The attainable advantage to this property of a locking plate�screw system is a decreased incidence of inflammatory issues from loosening of the hardware. It is understood that unfastened hardware propagates an inflammatory response and promotes infection. For the hardware or a locking plate� screw system to loosen, loosening of a screw from the plate or loosening of all the screws from their bony insertions must occur. A third advantage to a locking screw�plate system is that the amount of stability offered across the fracture gap is bigger than when standard nonlocking screws are used. However, given the potential benefits that locking plate�screw methods provide, such techniques must be considered each time noncompression plates are chosen for a fracture. To apply the lag screw method, two sound bony cortices are required because this system shares the hundreds with the bone. As with using compression bone plates, lag screw fixation is a technique that should be used only to provide absolute inflexible fixation. Note the second set of threads just under the head of the screw that can lock in to receptacle threads inside the outlet of the bone plate. A, the outer cortex is drilled to the exterior diameter of the screw threads and is countersunk to receive the top of the screw. It uses less hardware in comparison with the use of plates, thus making it less expensive. One must understand fully that the lag screw technique of fixation is one that depends on compression of bone fragments.
References
- Wolf DG, Greenberg D, Kalkstein D, et al. Comparison of human metapneumovirus, respiratory syncytial virus and Influenza A virus lower respiratory tract infections in hospitalized young children. Pediatr Infect Dis J 2006;25:320-4.
- Yao KA, Hsueh EC, Essner R, et al. Is sentinel lymph node mapping indicated for isolated local and in-transit recurrent melanoma? Ann Surg 2003;238(5):743-747.
- Weber DM, Chen C, Niesvizky R, Wang M, Belch A, Stadtmauer EA, et al. Lenalidomide plus dexamethasone for relapsed multiple myeloma in North America. N Engl J Med 2007;357(21):2133-2142.
- Ramana RK, Ronan A, et al. Long - term clinical outcomes of real - world experience using sirolimus - eluting stents in saphenous vein graft disease. Catheter Cardiovasc Interv 2008; 71:886.
- Werdnig G. Zwei fruhinfantile hereditare falle von progressiver muskelatrophie unter dem bilde der dystropine, ager auf neurotischer grundlage. Arch Psychiatr. 1891;22:437-481.
- Huber AR, Kunkel SL, Todd RF 3rd, Weiss SJ: Regulation of transendothelial neutrophil migration by endogenous interleukin-8, Science 254(5028):99-102, 1991.