Michael D. Katz, PharmD
- Professor, Department of Pharmacy Practice and Science, The University of Arizona College of Pharmacy, Tucson, Arizona

https://www.pharmacy.arizona.edu/directory/profile/michael-katz-pharmd
Renagel dosages: 800 mg, 400 mg
Renagel packs: 10 pills, 30 pills, 60 pills, 120 pills, 90 pills

Renagel 800 mg low price
Sonography could prove more and more useful to diagnose adhesive capsulitis because of its low price, portability, and lack of ionizing radiation. This may help the affected person put together for a sluggish progression and allay some of their concerns. Patients also wants to be made conscious of the significance of preserving or bettering motion on a symptom-limited basis. Aggressive, painful stretching is often poorly tolerated by these patients and should exacerbate the synovial pathology and subsequent fibrosis. For many sufferers, pain is a extra vital concern than lack of shoulder operate. Randomized scientific trials comparing adhesive capsulitis remedy outcomes are sparse and usually involve few sufferers. Lack of standardization of treatment approaches makes it tough to determine which interventions or mixture of interventions are efficacious. A pattern rehabilitation program for adhesive capsulitis is offered at the end of the chapter. Differences in reported success rates with numerous interventions could additionally be attributable to the timing of remedy. Patients in the end stage of adhesive capsulitis could experience improvement no matter intervention because of pure development of the illness. This suggests that corticosteroids have a therapeutic impact on the synovial pathology, maybe by quelling synovitis or by inhibiting synovial angiogenesis. Immediate enchancment in glenohumeral motion is widespread after injection, but this enchancment may be attributable to the impact of anesthetics that are sometimes injected together with the corticosteroids. The effectiveness of corticosteroid injections in bettering movement and decreasing pain appears to be most profound in the first 3�4 weeks in sufferers with adhesive capsulitis. Injections might augment the efficacy of supervised physical remedy, however this effect additionally appears short-lived. Oral steroids can also have some profit, though information recommend that worthwhile advantages are more likely to be short-lived. Still, oral or injected steroidal/nonsteroidal medications, together with stretching and mobilization methods to increase extensibility of the glenohumeral joint capsule, must be thought of for initial treatment. The vigor of stretching and mobilization must be titrated in accordance with affected person irritability. Diercks and Stevens (2004) reported that sufferers with adhesive capsulitis who stretched under the onset of pain fared higher than patients who stretched beyond their pain threshold. Moist hot packs or warm-water immersion may be utilized to promote rest and tissue extensibility prior to, or throughout, mobilization or stretching workout routines. Jewell and colleagues (2009) reported that the use of iontophoresis, phonophoresis, ultrasound, or massage decreased the likelihood of improvements in pain or perform by 19% to 32% in sufferers with adhesive capsulitis, suggesting that use of those interventions must be minimized. Patients with reasonable irritability expertise ache and stiffness which are roughly equal. Patients in this research were instructed to exercise 5 instances each day, but common compliance was twice every day. Other research have additionally proven that day by day train is apt to be effective in relieving symptoms with adhesive capsulitis. Of interest, 91% of sufferers in the Griggs examine also had supervised bodily remedy twice weekly. Still, numerous further research suggest that sufferers treated with joint mobilization, with or with out concurrent interventions, are probably to have better outcomes. On the opposite end of the spectrum, patients with low irritability who experience stiffness greater than ache ought to reply favorably to extra aggressive mobilization and stretching, closed manipulation, or surgical release to accelerate restoration. Clinicians trying to regain shoulder exterior rotation ought to carry out stretching and joint mobilization methods that focus on the rotator interval and coracohumeral ligament. These structures constrain inferior humeral head translation and external rotation with the arm in neutral. Anecdotally, I have found that inferior and posterior gliding mobilizations for the proximal humerus tend to be much less irritating and more effective than external rotation stretching or anterior gliding mobilizations in sufferers with adhesive capsulitis. Patients with more severe pain and practical limitations at the initiation of remedy are inclined to have poorer outcomes with conservative care.
Buy discount renagel 400 mg on-line
Young, athletic populations are at even higher threat, with a examine of cadets at the United States Military Academy demonstrating an overall incidence of shoulder instability of 2. In this inhabitants, trauma was recognized as the commonest etiology, with more than 85% of sufferers reporting antecedent trauma. More than 90% of shoulder dislocations are within the anterior path, particularly as a result of the place of mixed external rotation and abduction, widespread in many contact sports, locations the shoulder in an especially vulnerable place. Most regarding relating to first-time shoulder dislocations is the high recurrence rate, which has been reported as between 20% and 50% and as high as 90% in younger patients. These epidemiologic findings spotlight the significance of accurately figuring out and appropriately treating shoulder instability. There continues to be, nevertheless, considerable controversy concerning acceptable treatment algorithms for shoulder instability. Prior to deciding on an appropriate treatment course, factors including affected person age, type of activity/sport, activity/sport degree, objectives, and chance of compliance must be thought of. In addition, the mechanism of injury and the kind of damage incurred, which can embrace labral, capsule, biceps, and/or rotator cuff lesions, along with bony avulsions, will influence probably the most applicable course of therapy for the affected person. Understanding these factors will allow the treating clinician to decide (1) whether nonoperative versus operative treatment is indicated, and (2) if operative intervention is required, what form this could take. In this part we briefly review the anatomy and biomechanics of the glenohumeral joint, describe the classification of instability events, talk about the out there nonoperative and operative interventions for treating the spectrum of instability disorders, and provide rehabilitation protocols. The glenoid fossa is a shallow structure, masking only 25% of the humeral head surface. Stability in the joint is due to this fact primarily a consequence of its static and dynamic stabilizers. The static stabilizers consist of the bony anatomy, the glenoid labrum, and capsular and ligamentous complexes and are sometimes solely improved with surgical intervention as soon as injured. The dynamic stabilizers, together with the rotator cuff muscle tissue and long head of the biceps tendon, can often be improved with an appropriate nonoperative rehabilitation program after an instability event. In truth, correct strengthening of the rotator cuff musculature and scapular stabilizers are important elements of any rehabilitation protocol, together with those for nonoperative management of shoulder instability and a half of the rehabilitation following surgical procedure. It is particularly important to note the integrity and condition of the subscapularis with regard to rehabilitation following shoulder surgery. Ensuring excellent communication with the surgical staff and the postoperative rehabilitation group of exactly what was performed through the surgical procedure is important to postoperative success. Instability is symptomatic laxity-as all shoulders have and require some degree of laxity to transfer through a functional arc of motion. Similar to different joints, shoulder instability varies in severity from microinstability to subluxation and in the end to frank dislocation. Microinstability refers to pathologic movement of the humeral head, most often in a quantity of directions, secondary to generalized capsular laxity. Subluxation denotes translation of the humeral head past regular physiologic limits while still sustaining contact with the glenoid. Dislocation differs from subluxation in that the translation of the humeral head is critical enough to utterly disassociate the articular surfaces of the humerus and the glenoid; this magnitude of instability will commonly require handbook reduction. Shoulder instability is usually described in relation to the course of the instability event: anterior, posterior, and multidirectional. Anterior instability is the most common manifestation of unidirectional instability, comprising greater than 90% of shoulder dislocations. This sort of harm mostly occurs as the outcome of a one-time traumatic episode to a shoulder in a vulnerable place of combined abduction and external rotation. The damage may involve an avulsion of the anteroinferior labrum from the glenoid, commonly referred to because the Bankart lesion. Occasionally a fragment of the underlying glenoid rim also may be fractured off; this lesion is referred to as a bony Bankart lesion. Posterior instability is much less frequent than anterior instability, accounting for 2% to 10% of shoulder dislocations. Posterior dislocations are sometimes related to axial loads utilized to the adducted arm and are classically associated with electrocution and seizures. Structural adjustments related to posterior instability embody avulsions of the posterior labrum (a reverse Bankart lesion), which can be associated with a posterior glenoid rim fracture.
Order discount renagel
Starting position is with the shoulder within the impartial position of 0 degrees of forward flexion, abduction, and external rotation. Nonoperative Management of Anterior Shoulder Instability 167 Nonoperative Management of Anterior Shoulder Instability (Continued) � Minimal pain or tenderness with strengthening exercises. Advance to dynamic stabilization by performing a push-up on an unstable floor (pictured), a "plyo" or weighted ball, when applicable. Continued on following web page 168 Shoulder Injuries Nonoperative Management of Anterior Shoulder Instability (Continued) Goals � Prepare for gradual return to practical and sporting activities. Recurrent instability as outlined by three or extra instability events inside a yr, or instability that occurs at rest or throughout sleep, is a powerful indication for surgical administration. Pain Control � Understand management after surgical manipulation of subscapularis. Immobilization � Sling immobilization: 2 to 4 weeks duration-during day and especially at night. Following an Arthroscopic Anterior Surgical Stabilization Procedure 169 Following an Arthroscopic Anterior Surgical Stabilization Procedure (Continued) � Internal rotation. Note: For overhead athletes, the movement objectives should be inside 10 levels of regular for the affected shoulder. Continued on following web page a hundred and seventy Shoulder Injuries Following an Arthroscopic Anterior Surgical Stabilization Procedure (Continued) Progressive, systematic interval program for returning to sports: same as Rehabilitation Protocol 3-5. Maximum improvement is predicted by 12 months; most patients can return to sports activities and full-duty work standing by 6 months. Therapist or athletic coach will manually facilitate correct glenohumeral to scapular motion ratio. Immobilization � Sling immobilization: 0 to four weeks duration-during day and particularly at night time. Wean at week 2 as tolerated however should be worn throughout sleep for minimum of 2 weeks. Progress oscillation train in forty five degrees of glenohumeral joint abduction, ninety levels of abduction, ninety levels of flexion, and a hundred forty five degrees of scaption. Arthroscopic Anterior Shoulder Instability Protocol 173 Postoperative Rehabilitation After Open (Bankart) Anterior Capsulolabral Reconstruction (Continued) � Progress plyometrics to one handed (dribble). Range of Motion � Progress passive forward flexion 150 degrees, scapular 150 degrees, and abduction 100 levels. Nonoperative Posterior Instability Protocol one hundred seventy five Nonoperative Posterior Instability Physical Therapy Treatment Guidelines (Continued) � Wrist flexion/extension. Phase Ivb: Weeks 10�12 Goals � Increased scapular stabilizer and rotator cuff strength. Phase v: Weeks 13�16 Goals and Precautions � Initiate sports activities specific training exercises. Continued on following web page 178 Shoulder Injuries After Posterior Shoulder Stabilization (Continued) Restrictions � Shoulder movement: lively and active-assisted motion workout routines. Progressive, Systematic Interval Program for Returning to Sports � Maximum enchancment is anticipated by 12 months. Continued on following web page a hundred and eighty Shoulder Injuries After Open Inferior Capsular Shift for Multidirectional Instability (Continued) Upper Extremity Endurance Training � Incorporated endurance training for the higher extremity. Progressive, Systematic Interval Program for Returning to Sports � Refer to phase V of Rehabilitation Protocol 3-5. Treatment of Complications � Refer to outline in phase V of Rehabilitation Protocol 3-5. Individual variations will occur primarily based on patient tolerance and response to treatment. Evans L, Hardy L: Injury rehabilitation: a qualitative follow-up research, Res Q Exerc Sport seventy three:320�329, 2002. Hayes K, Callanan M, Walton J, et al: Shoulder instability: management and rehabilitation, J Orthop Sports Phys Ther 32:497�509, 2002. Itoi E, Hatakeyama Y, Kido T, Sato T, Minagawa H, et al: A new technique of immobilization after traumatic anterior dislocation of the shoulder: A preliminary research, J Shoulder Elbow Surg 12(5):413�415, 2003.
Purchase discount renagel online
Nevertheless, he adopted the results from medical research that was relevant to his clinical work. Additionally, he was experienced in carrying out autopsies since his medical student days, and continued pathological examinations when practising medication to help study the structural and practical effects of diseases. This included his interest in brain and behaviour (topic updated in earlier pages). Where indicated, he practised the holistic method of addressing the mind together with the physique as the ancient Greek physicians had carried out. This specific method was needed within the management of sure diseases such as anorexia nervosa, which stays a modern-day scourge (see Chapter 4). His expertise in applying the mind�body approach for profitable therapy outcomes consists of the documented case of a girl who was unable to walk for 3 years, despite many treatments, due to her complaint of paralysis of her legs. She began strolling after he treated her for two weeks, when he made her believe that she might achieve this, again suggestive of a psychosomatic methodology of remedy for such illnesses; this is additionally in evidence right now (see Chapter 4). His interest in furthering pathology in order to perceive the pure history of the illness made him gather pathological specimens, and then go away his collection for future learning; his curiosity in teaching medicine made him depart his cache of books to a library; a present to posterity. Consequently, its wider application to affected person care or associated analysis petered out when the native enthusiasm had waned. Meanwhile, technological advances focussing primarily on the bodily side of illnesses led to a mind�body dualism in medical administration by marginalising the psychosocial aetiological components. A turf-war between specialties was created with many sufferers failing to get reduction once they had a clinical condition with a twin pathology however well being professionals thought-about one facet solely. The Systems Theory [60,62] is being mentioned here, because it pertains to one other twentieth century idea of psychosomatic medicine. It was introduced in 1958 by Adolf Meyer, and after that it was endorsed by Leon Eisenberg (1995). Additionally, in 1977, Herbert Weiner emphasised that within the understanding of illness, not solely should the organic, psychological, and social aspects be linked however they should even be associated on the genetic, molecular, and neurophysiological levels. Stress is a quantity one aetiological environmental issue within the modern social setting that can lead to multi-organ injury with deleterious results. Recent studies point out that its results can generate each physical and psychological symptoms as a result of neurogenic inflammation arising from the discharge of cytokines in addition to influencing the immune privilege of the endothelial cells of the blood�brain barrier [65]; this impedes effective functioning. Exposure to any stressor, whether a psychological stress, central nervous system injury/infection, or neurological illness, ends in proinflammatory responses via neuropeptides, cytokines, and stress hormones of the central nervous system; this results in a quantity of mental well being problems. The relationship of stress to disease was first studied systematically by Walter Cannon (1875�1945). That mentioned, in the habitually suave one that can do neither, such stress may end up in cardiovascular or neuroendocrine responses that can cause appreciable morbidity with sometimes, grave sequelae. The common adaptation syndrome was the model of stress developed by Hans Selye (1907�1982). This consisted of the alarm reaction in the 1st stage of resistance to stress, adopted by adaptation in the 2nd stage, and finally exhaustion within the 3rd stage. The nonspecific Stress Theory suggests that continual stress can even lead to nervousness that can have a deleterious effect on the functioning of many organs. This can lead to a susceptibility to organ harm however this susceptibility could also be due to the action of environmental components or a attainable genetic vulnerability. Moreover, multiple stressors occurring even over a short time frame or chronic stress as a outcome of a single stressor that acts for a protracted interval can have main repercussions. Perception of severe stress corresponding to that related to sudden assault, even when solely a single episode is experienced, can have long-lasting sequelae (see Chapter 12). There is a few proof that those that face stress optimistically rather than pessimistically are less likely to expertise psychosomatic issues, and recovery might be simpler for them. It can be recognised that implementing biopsychosocial patient-centred care, including particular psychotherapy could be helpful in the restoration from the dangerous effects of stress. Further attention to the necessity for the event of psychosomatic awareness, and selling the ongoing pattern for its application to patient care, is taken into account here. Promoting the psychosomatic strategy in futuristic clinical follow Medical ideas in the twentieth century appeared to have set the development in thinking in path of a patient-centred strategy [67] for the management of many modern-day diseases. This has gained floor over time as contemporary scientific practice along with affected person selection have advocated this [68,69]. Although this seems perplexing for these unaccustomed to offering patient-centred, psychosomatic healthcare, the method was followed even by many historic medical practitioners, who have been able to obtain passable outcomes [33]. The concept of mind�body interplay grew to become unpopular in medieval instances, and was neglected with the arrival of the commercial age but appears to have made a comeback [1].
Buy 400 mg renagel amex
In each a cadaver biomechanical study and an in vivo examine in adults, Laprade et al. Full weightbearing with quadriceps and hamstring strengthening is encouraged once the pain has subsided. No potential randomized (level 1) research have in contrast repair and reconstruction. Each functional objective have to be attained before the athlete can progress into the following phase. Shelbourne and Dickens (2007) found 88% of sufferers who underwent partial medial meniscectomy had joint house narrowing of two mm or much less at a mean followup of 12 years. Meniscal Healing King, in 1936, first noted that communication with the peripheral blood supply was important for meniscal therapeutic. Arnoczky and Warren, in 1982, described the Anterior cruciate ligament Transverse intermeniscal ligament Medial collateral ligament Medial meniscus Lateral meniscus Ligament of Wrisberg Posterior cruciate ligament A Superficial cells Superficial zone Radial tie fibers Deep zone meniscal movement the lateral meniscus has been proven to be more cellular than the medial meniscus. The decreased mobility of the posterior medial meniscus may result in higher stresses on this space, leading to elevated vulnerability to damage. This would explain the higher rate of meniscal tears that occur within the posterior medial meniscus. Weightbearing has been proven to impact few changes in the motion of the menisci, although it has been advised that meniscal loading could lead to distraction of radial tears. Clinically, second-look arthroscopy has proven that extension of the knee maintains a posterior horn meniscal tear in a reduced position, and knee flexion results in displacement of the tear. Random collagen fibers Circumferential collagen fibers Deep cells B determine 4-58 A, Anatomy of the menisci considered from above. The illustration demonstrates the collagen fiber orientation within the surface and deep zones. Superficial meniscal cells tend to be fibroblastic, whereas the deep cells have a rounded morphology. In children, the peripheral blood vessels permeate the complete thickness of the meniscus. It is in this vascular region that the healing potential of a meniscal tear is best. This potential drops off dramatically as the tear progresses away from the periphery. Longitudinal tears have a extra favorable healing potential compared with radial tears. Traumatic tears have higher therapeutic charges than degenerative tears, and acute tears heal higher than continual tears. Several studies have confirmed the benefits of early movement by demonstrating meniscal atrophy and decreased collagen content in menisci after immobilization. This elevated translation may place detrimental stresses throughout a therapeutic meniscus. The combination of weightbearing and increasing knee flexion must be carefully balanced within the improvement of a rehabilitation protocol. Patients with limb malalignment tend to have more degenerative meniscal tears, which have been instructed to have an inherently poorer therapeutic capacity. The use of an "unloader" brace has been beneficial to help protect the therapeutic meniscus, although no scientific information exist to support this method. T determine 4-59 Scan of 5-mm thick frontal section of the medial compartment of the knee (Spalteholz 3�). Rehabilitation After Meniscal Repair Vertical tear Horizontal tear (splits meniscus parallel to tibial plateau) Radial tear Oblique tear Complex (degenerative) tear determine 4-60 Variousmeniscustears. In tears with decreased therapeutic potential (such as white�white tears, radial tears, or complicated sample tears), limiting weightbearing and limiting flexion to 60 levels for the primary 4 weeks have been instructed to higher defend the repair and increase the therapeutic potential of those tough tears. Patellofemoral Disorders 263 A B determine 4-61 A, Arthroscopic partial meniscectomy of a bucket-handle tear of the meniscus. This often ends in a locked knee, which manifests as the shortcoming to extend (straighten) the knee the last 5 to 15 degrees.
Buy renagel 400mg lowest price
Considerable controversy exists over the suitable preliminary therapy for sufferers with instability. There is general settlement, however, on the appropriate remedy for an acute shoulder dislocation. Any unreduced dislocation should bear closed discount with radiographic confirmation of reduction. In basic, the shoulder should be reduced as quickly as potential using a wide range of well-described discount techniques. Special Considerations � First-time dislocator: � Overall, the nonoperative remedy options for sufferers following first-time shoulder dislocation are controversial, and regardless of the treatment, reported recurrence charges are high, especially for young, extremely energetic patients. The preliminary results reported with immobilization in external rotation are fascinating; nonetheless, larger, longer-term clinical Nonoperative Treatment and Rehabilitation Nonoperative treatment protocols typically encompass immobilization adopted by rehabilitation with an skilled physical therapist. Traditionally, following 110 Shoulder Injuries research are needed earlier than any single immobilization technique may be universally recommended. Specifically, in sufferers youthful than 20 years old with a one-time acute shoulder dislocation treated nonoperatively, recurrence charges have been reported as high as 90%. The authors discovered that 26 of the 30 sufferers have been able to return to play and complete the season after approximately 10 days of missed time; nevertheless, 37% skilled no much less than one episode of recurrent instability through the season. Further, 16 athletes required surgical intervention following their aggressive season. Thus, the therapy of a dislocation in an in-season athlete is mostly to end the season (possibly with the usage of an exterior rotation protection brace) after which think about surgery once the season is completed. However, recurrences through the season after an preliminary dislocation require extra careful discussions with the athlete for his or her wishes and return-to-play capability. In the open procedure, the labrum is anatomically reduced and repaired to the anterior glenoid. Given the common coexistence of capsular harm and stretch, a concomitant capsular shift procedure is usually carried out. Various methods for the capsular shift have been described; the important underlying objective is to restore the injured anteroinferior capsule and labral restore. Although initial reviews described the next recurrence fee after arthroscopic restore, current research have proven that recurrence charges are practically comparable to open repair, particularly in those sufferers with out important glenoid bone loss or different structural abnormalities. With the ultimate word focus of regaining after which sustaining shoulder stability, the goals of postoperative rehabilitation commonly concentrate on avoiding common Postoperative remedy and rehabilitation Anterior Instability Traumatic dislocations are often related to vital structural damage. In these sufferers, operative remedy has been shown to have a decrease risk of recurrent dislocation as compared to nonoperative remedy. Patients with vital bone injury-glenoid defects (20% to 25% or more), displaced tuberosity fractures, and irreducible dislocations-should be handled with operative stabilization. Other indications for operative intervention embrace three or extra recurrent dislocations in a yr and dislocations that happen at relaxation or throughout sleep. The open Bankart restore was as quickly as considered the gold commonplace within the therapy of anterior shoulder instability; however, proper affected person choice combined figure 3-34 An arthroscopic image of an anterior labral tear (soft tissue Bankart) (black arrows). Shoulder Instability Treatment and Rehabilitation 111 complications following anterior stabilization procedures. Posterior Instability the initial remedy for posterior instability is often nonoperative, particularly in the case of an atraumatic etiology, as a end result of profitable outcomes following nonoperative therapy in atraumatic subluxators have been reported. Appropriately planned strengthening packages have been proven to be efficient in augmenting stability and decreasing pain, especially for patients affected by laxity secondary to repetitive microtrauma. However, the efficacy of nonoperative remedy in treating traumatic posterior dislocators is significantly decrease, estimated at roughly 16%. Indications for surgical remedy subsequently embrace the frequent sequelae of traumatic dislocations, together with posterior glenoid rim fractures greater than 25%, displaced lesser tuberosity fractures, reverse Hill-Sachs lesions of greater than 40% of the humeral head, recurrent instability episodes, and irreducible dislocations. Patients with mechanical symptoms additionally usually respond poorly to conservative therapy and thus may be indicated for surgical therapy. Failure of 3 to 6 months of conservative therapy can be a sign for operative restore. The most typical presenting grievance in a affected person with posterior shoulder instability is pain and pain with provocative workouts (the arm in flexion and inner rotation), corresponding to bench press, push-ups, and presses. Specific operative therapy methods for posterior instability are comparable in theory to the therapies for anterior instability.
Cheap renagel 800mg line
The estimated cumulative survival probabilities at each time point in the study can be then plotted on the y-axis towards time on the x-axis to give a survivor perform or plot. Risk is determined by the likelihood of creating disease, given the presence or absence of a danger factor. It is estimated through the use of the incidence of disease development in a gaggle having the risk factor or publicity of interest. Several methodologies are used to compare survival plots between two research populations. These embody the Mantel-Haenszel methods, the log-rank test, and the weighted log-rank exams. Implicit in these methods is the assumption that the chance of a examine outcome. Therefore, understanding the power of a medical or laboratory check to either confirm or rule out a analysis is essential for practitioners. Epidemiologic assessments help evaluate the reliability and usefulness of exams used to diagnose illness. In a inhabitants of sufferers known to have or not have a illness of curiosity, each is run a diagnostic test to detect disease. The first is the power of a take a look at to correctly identify persons with illness after they have it. At every time point, a progressively smaller proportion of the study inhabitants is free of illness. Because subjects are evaluated only on a yearly basis for disease, the chance of being freed from disease at intermediate time factors is assumed to be the identical because the likelihood during the last yr of evaluation. In addition, many study subjects could also be censored out of a cohort examine for reasons other than the event of the top point of interest. Dealing with these people typically means making the assumption that they left the examine at the mid-point of each time interval. This method for dealing with those who left the examine for causes aside from disease incidence is legitimate only if censoring happens uniformly through each study interval and the danger for disease (or death) at any time is uniform all through the whole study interval. Using this step-wise strategy to survival evaluation typically leads to overestimation of survival probabilities at a time level between examine intervals. Progressively shortening the time intervals in which the population is assessed for the result could help mitigate some of these limitations. A methodology of doing just this is exemplified by the Kaplan-Meier method to survival evaluation. In the Kaplan-Meier strategy, study time intervals are outlined primarily based on the time point at which a topic develops disease. This leads to a survival plot with essentially the most possible time intervals of the shortest duration and helps minimize the problems with the way to deal with the data from examine withdrawals. The Kaplan-Meier approach maximizes the info that can be utilized to assemble the survival plot. This will increase the facility for At instances, what practitioners actually wish to know is the likelihood that a affected person has a disease if the ordered take a look at comes Table fifty three. These test statistics are often identified as the optimistic predictive worth and unfavorable predictive worth, respectively. If we try to compare the performance of several checks without delay, one metric that might be used is the chance ratio. The likelihood ratio is calculated as the sensitivity of a check divided by (1 � specificity). An improve in sensitivity or specificity could improve the probability ratio of a test. Tests a and b, respectively, have proportionally greater sensitivities for a given specificity. However, combining the 2 checks collectively as a composite might give the perfect diagnostic take a look at for the illness y. The training pediatric nephrologist should be properly versed in lots of of these ideas to correctly interpret both the relevance and high quality of studies as relevant to their own sufferers.
Buy renagel mastercard
Given that the average runner may have 800 to 2000 footstrikes per mile, the chance for harm to occur is critical. These information point out that running has in reality become a significant well being care concern. The variety of individuals is rising, and a big percentage of these participants will become injured. Health care providers can then not only present effective technique of treatment should an injury happen, but in addition present efficient damage prevention packages. Gait: Walking and Running the gait cycle has been outlined by Thordarson (1997) as the interval from initial contact of one foot until the initial contact of that same foot. A temporary evaluate of the gait cycle will provide some background on the nature of mechanical loading and the neuromuscular necessities of each walking and running. Running Mechanics the walking gait cycle consists of two phases, stance and swing. During preliminary contact, the loading response commences as forces are managed eccentrically. Once the center of gravity is directly over the stance foot, terminal stance begins. Stance section can also be considered by way of useful components-the absorption of forces on loading, adopted by the propulsion of the physique forward. During the swing section of gait, preliminary swing begins at toe off and continues till the knee reaches a maximal knee flexion of roughly 60 levels. Midswing follows and continues until the decrease leg/ shank is perpendicular to the bottom. The stance phase might contain an preliminary foot contact which takes place as a heel strike, midfoot strike, or forefoot strike. Initial foot contact exists on a continuum with increasing gait velocity, progressing from heel strike in strolling to forefoot strike in sprinting. The share of the gait cycle 393 394 Special Topics Table 7-1 Incidence of Injuries by Body Area anatomic Region Knee Shin, Achilles tendon, calf, heel Foot and toes Hamstring, quadriceps Percentage of injuries 7. [newline]Incidence and determinants of lower extremity running accidents in lengthy distance runners: A systematic evaluation. Equivalent exertion spent in the stance phase varies relying on gait speed-60% with strolling, 40% with working, and just 22% with world class sprinters. The walking gait cycle is distinct in that it involves a interval of double limb help during which each of the ft are on the bottom. The running gait cycle is distinct in that it involves a period of double float by which both of the ft are off the ground. The development from walking gait to running gait is a continuum-from double limb support in walking to double float interval in operating. The speed at which this transition occurs varies between people, although it tends to be at or close to a velocity of 12:00 per mile (5. This becomes an essential issue when 70% of the operating population runs at a pace of 10:00 per mile or slower. Though quick walking and sluggish jogging have an identical cardiovascular response, gradual jogging creates floor response forces and loading rates as a lot as 65% higher than fast walking (Table 7-2). RunSmart: A Comprehensive Approach to Injury-Free Running, Morrisville, 2008, Lulu Press. Running and sprinting require extra energy and vary of movement on the hip, knee, and ankle as speed is increased. During the working gait cycle, the preliminary practical task of the stance leg is absorption-to eccentrically decelerate and stabilize the limb-before concentrically activating the lower limb for propulsion. Relationship between vertical ground response pressure and velocity during walking, slow jogging, and running. This two-peaked configuration of the ground reaction curve is constant within the literature for heel-strike runners. Ground reaction forces seem to increase linearly up to a gait speed of 60% of maximum pace (average of 4. It is also noteworthy that in running, athletes that heel strike upon preliminary contact have a higher initial peak in vertical ground response force than midfoot strikers. For a runner who has a heel strike, these forces transmit immediately via the heel and, therefore, are attenuated by the heel fat pad, pronation of the foot, and primarily passive, greater than active, mechanisms in the decrease extremity. However, for a runner with a midfoot or forefoot strike, these forces are primarily attenuated by the eccentric activation of the gastrocemius/soleous advanced, the quadriceps, and to a lesser degree, the pronation of the foot.
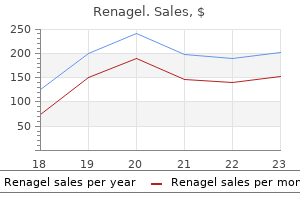
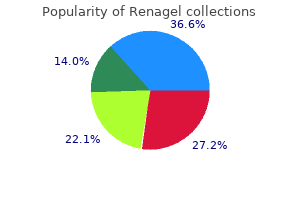
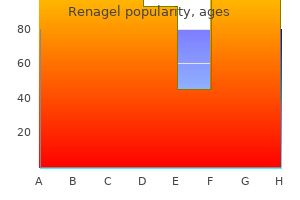
Real Experiences: Customer Reviews on Renagel
Irhabar, 61 years: Plantar pressure total main symmetry measured throughout squat to 90� knee flexion (20% discrepancy between sides) three.
Onatas, 39 years: These information indicate that operating has in reality turn out to be a major well being care problem.
8 of 10 - Review by R. Nerusul
Votes: 72 votes
Total customer reviews: 72
References
- Angelini P, Velesco JA, Flamm S. Coronary anomalies: incidence, pathophysiology, and clinical relevance. Circulation. 2002;105:2449-2454.
- Osler T, Baker SP, Long W. A modifi cation of the injury severity score that both improves accuracy and simplifi es scoring. J Trauma. 1997;43(6);922-926.
- Elraiyah T, Sonbol MB, Wang Z, et al: The benefits and harms of systemic dehydroepiandrosterone (DHEA) in postmenopausal women with normal adrenal function: a systematic review and meta-analysis, J Clin Endocrinol Metab 99(10):3536n3542, 2014.
- Jonsson Funk M, Levin PJ, Wu JM: Trends in the surgical management of stress urinary incontinence, Obstet Gynecol 119:845n851, 2012.
- Geller A, Wang KK, DiMagno EP. Diagnosis of foregut duplication cysts by endoscopic ultrasonography. Gastroenterology. 1995;109:838-842.
- Bader, P., Burkhard, F.C., Markwalder, R. et al. Is a limited lymph node dissection an adequate staging procedure for prostate cancer? J Urol 2002;168:514-518.
- Young WF, Stanson AW, Thompson GB, et al. Role for adrenal venous sampling in primary aldosteronism. Surgery 2004;136(6):1227-1235.
- Sun Y, Gan TJ, Dubose JW, Habib AS. Acupuncture and related techniques for postoperative pain: a systematic review of randomized controlled trials. Br J Anaesth. 2008;101(2):151-160.